Medicare Questions – Answering the Most FAQ
Nationwide Blog | November 10, 2022 | Medicare | Medicare Insurance | Start A Quote Today!
Key Takeaways:
- Many people don’t realize that Medicare decisions can have financial implications, and Medicare costs can be incorporated into comprehensive financial planning.
- “When and how can I enroll in Medicare?” “How much does Medicare cost and what does it cover?” are all common questions you may have regarding your health care plan for retirement.
- In addition to working closely with your financial planner, you can assess specific Medicare drug and health care plan costs by utilizing online tools.
Every day, around 10,000 members of the Baby Boomer Generation turn age 65, which is generally the age they become eligible for Medicare. [1][2] Often, this is the first time that many Baby Boomers realize that decisions around Medicare aren’t just medical decisions; Medicare decisions also have significant financial implications. Once you come to this realization, you can turn to the financial professionals on whom you depend to help make sense of Medicare and in turn help you make financially sound Medicare decisions.
Understanding Medicare can be difficult, but the Nationwide Retirement Institute® is here to help you by sharing some of the most common Medicare questions. Working with a financial professional and utilizing various planning tools can help you incorporate Medicare costs into your financial plan.
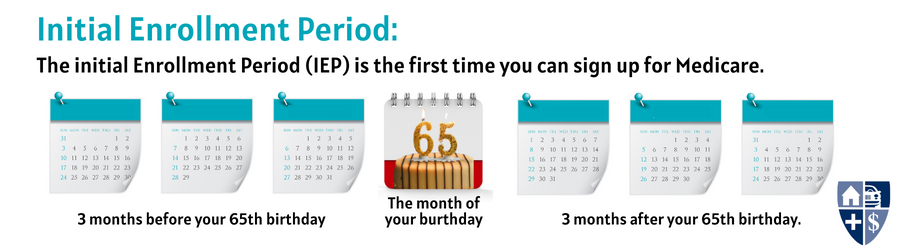
When do I enroll in Medicare?
For everyone who turns 65 and is eligible for Medicare, there’s a seven-month “initial enrollment period,” or IEP. The IEP spans from the start of the third month before your 65th birthday through the end of the third month following the month of your 65th birthday. This IEP is available regardless of whether you continue to work past age 65.
If you choose to work past age 65 and remain eligible for group health coverage provided by your employer (or your spouse’s employer), then you may choose not to enroll in Medicare during your IEP. If this is the case, you’ll have a second chance to enroll during a “special enrollment period,” or SEP. The SEP generally lasts 8 months, beginning from the month after your employment or group health coverage ends, whichever occurs first. If you do not enroll in Medicare during your IEP or SEP, then you must wait to sign up during the General Enrollment Period between January 1st and March 31st of each year; but beware that in this circumstance, you may be subject to lifelong penalties in the form of increased premiums once you do enroll.
How do I enroll in Medicare?
That depends.
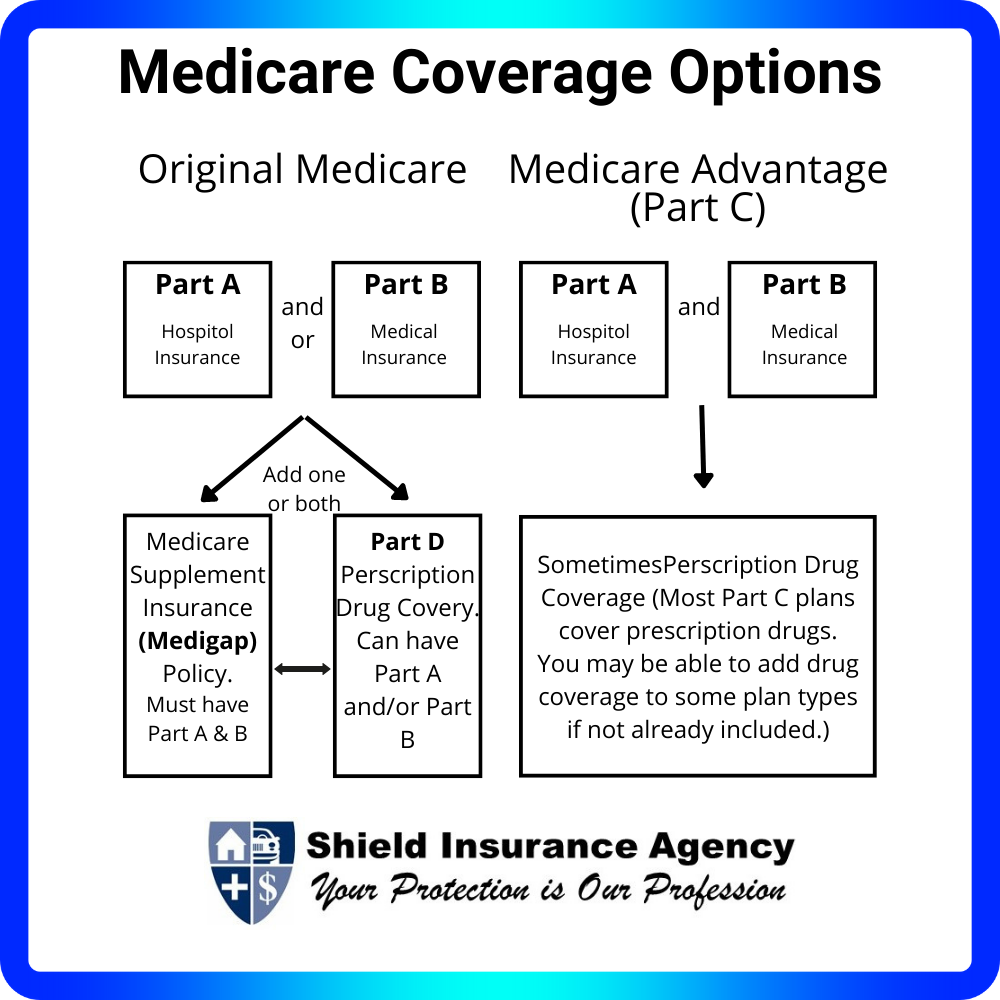
If you are already receiving Social Security when you turn 65, you will automatically be enrolled in Original Medicare, which means Medicare Parts A & B. Your eligibility will be effective the first day of the month you turn 65. You will not even need to sign up. You should simply receive a red, white, and blue Medicare card in the mail around three months before your 65th birthday.
If you choose to stay on Original Medicare, you will likely want to proactively enroll in a Medicare Part D plan as well, to get prescription drug coverage. In the alternative, you may choose to enroll in a Medicare Advantage Plan, which is known as Medicare Part C. Medicare Advantage plans to replace Original Medicare and Medicare Part D, but you must proactively enroll in Medicare Advantage plans as well. You can enroll in a Medicare Advantage Plan or a Medicare Part D plan during your IEP.
Medicare.gov/plan-compare shows specific Medicare drug plans and Medicare Advantage plan costs, and you have the opportunity to call the plans you’re interested in to get more details. For help comparing plan costs, the State Health Insurance Assistance Program (SHIP) can also assist you.
If you’re not already receiving Social Security at least 4 months before turning 65, you’ll need to sign up by:
- Applying online at Social Security. (If you start your online application and receive a re-entry number, you can go back to Social Security to finish your application at a later time.);
- Visit their local Social Security office; or
- Call Social Security at 1-800-772-1213 (TTY: 1-800-325-0778).
Nationwide teamed up with the National Council on Aging (NCOA) to create an unbiased tool to help sort through Medicare options. It’s called the NCOA My Medicare Matters® tool brought to you by Nationwide. The tool allows you to work with financial professionals so that they can assist you in the Medicare decision-making process before the completion of the enrollment process.
How much does Medicare cost?
That also depends. The first and most important thing to understand in the context of cost is that it will not be free! There are still premiums, copays, coinsurance, and deductibles to plan for.
If you sign up for Original Medicare, Part A will be free if you have paid at least 10 years of Medicare taxes. Part B will require a monthly premium of $170.10 in 2022. [3] That amount may be more if your income is high enough to cross certain thresholds.
Medicare Part D (for prescription drugs) and Medicare Advantage plans (Part C, an alternative to Original Medicare and Medicare Part D) will also have monthly premiums. The costs of those premiums will vary plan by plan and be impacted by other factors, like your age at enrollment and geographic location.
What does Medicare cover?
Not everything! That may be the simplest yet most important fact you need to understand. Medicare will not cover all medical care.
In particular, Medicare does not cover long-term care (LTC), nor vision or dental care. Also, Medicare does not cover care received outside of the USA. This means that supplemental insurance for LTC, dental and vision, and travel insurance, will be important to look into.
That being said, Medicare does cover most medical treatments and procedures. Original Medicare Parts A and B cover most basic medical services. In general, Medicare Part A covers hospitalizations (i.e., inpatient care) and Medicare Part B covers outpatient care. In addition to inpatient care, Part A also covers home healthcare in limited circumstances, as well as hospice care. Medicare Part B covers outpatient clinical services like doctor’s visits and emergency room visits, including observation. In addition to outpatient care, Part B also covers medical supplies (think splints and casts, or crutches or a wheelchair), X-rays and other radiology services, and preventive care and screening services. One important fact about this last category is that many of the preventive care and screening services covered under Part B are free; there is no coinsurance or other cost-sharing. Screenings for many cancers (including breast, cervical and vaginal, colorectal, and lung) are free, as are screenings for depression and diabetes. Many Medicare beneficiaries do not understand that these screenings, as well as many other preventive services (like flu shots), are free; consequently, they fail to seek out those services. It’s important for you to be aware of and take advantage of these free preventive and screening services to avoid delayed diagnosis and treatment of many different health conditions. Failing to do so can ultimately impact your longevity and quality of life, not to mention increase the eventual cost of treatment when an ailment’s symptoms appear later in a more advanced stage. As the adage goes, an ounce of prevention is worth a pound of cure!
Which Medicare coverage option is right for me?
For the third time in this blog, I must say it again: it depends. Decisions around Medicare are incredibly complex and depend on both medical and financial factors that are individual to each person. Many folks end up talking to their friends or neighbors for advice, but what works best for them may not work best for you! You should do some independent research and consult with your primary care physician or other medical professionals with whom you have an existing relationship so that you can make the most informed choices about the coverage and cost of your healthcare in retirement.
Where can I find out more?
If you want or need to learn more about Medicare, you can utilize other resources from Brianna, Shield Insurance Specialist. We are here to help answer all Medicare coverage questions.
GET IN TOUCH
Schedule a Visit
Medicare Questions to Ask Before Enrolling
Costs Associated with Medicare Coverage
Think ahead when choosing your Medicare plan
Sources:
[1] https://www.aarpinternational.org/initiatives/aging-readiness-competitiveness-arc/united-states
[3] https://www.medicare.gov/your-medicare-costs/part-b-costs
NFM-22483AO
Disclaimer:
This information is general in nature and is not intended to be tax, legal, accounting, or other professional advice. The information provided is based on current laws, which are subject to change at any time, and has not been endorsed by any government agency.
Nationwide and its representatives do not give legal or tax advice. Please consult an attorney or tax advisor for answers to legal questions.
My Medicare Matters® is a registered trademark of the National Council on Aging.
Nationwide and NCOA are separate and non-affiliated companies.
Nationwide Investment Services Corporation (NISC), member FINRA, Columbus, Ohio. The Nationwide Retirement Institute is a division of NISC.
Nationwide, the Nationwide N and Eagle, Nationwide is on your side, Nationwide Retirement Institute and other marks displayed in this message are service marks of Nationwide Mutual Insurance Company and/or its affiliates unless otherwise disclosed. Third-party marks that appear in this message are the property of their respective owners © 2022 Nationwide and Shield Insurance Agency
More interesting reads featured at the Shield Insurance Agency Blog
- Why Now Is a Smart Time for Michigan Businesses to Review Liability Coverage Before Spring Foot Traffic Increases
- Snowstorms and Roof Damage: Is Your Michigan Home Covered?
- Do You Need Recreational Insurance for Your Snowmobile in Michigan?
- The Importance of Giving Back During the Holiday Season
- Michigan Winter Driving: Essential Snow & Ice Safety Tips You Need to Know